
What is cancer?
Normally the cells that make up the body grow, divide, and replace themselves in an orderly manner. Sometimes, however, this order is upset and the cells divide abnormally to form cancerous cells.
Tumours can be either benign or malignant. Benign tumours are not cancer. They usually grow slowly, and generally do not spread to other parts of the body. Benign tumours can usually be removed surgically without any further problems. Malignant tumours are cancer. They are usually capable of invading adjacent tissues or metastasising (spreading) to other parts of the body. The most common methods for cancer to spread are through the lymphatic system to regional lymph nodes or through the bloodstream to distant organs.
How is cancer treated?
There are three major methods of treating cancer--surgery, radiation therapy, and chemotherapy.
Surgery involves the removal of the tumour and some of the surrounding normal tissues. This is a very localised form of treatment.
Radiation therapy involves the use of ionising radiation to destroy cancer cells. Radiation therapy is also a localised form of treatment. However, it is broader in scope than surgery because organs that cannot be removed surgically can usually be treated with irradiation.
Chemotherapy uses anticancer medication to destroy cancer cells. The drugs may be given by mouth, intramuscularly, or intravenously. Because the chemotherapy agents travel throughout the body, it can eradicate cancer cells in remote locations but at the same time cause damage to the body as a whole.
Many cancers are treated with a combination of these treatment modalities.
What is radiation therapy?
Radiation therapy is the careful use of high energy x-rays, gamma rays, or electrons to treat cancer. Radiation is effective in treating cancer because it damages cancer cells more than it does normal cells. However, normal tissues may also be damaged, which is one reason why side effects can occur. The goal of radiation therapy is to destroy the cancer with as little injury as possible to the surrounding normal tissues.
The purpose of radiation therapy is often to cure the patient of cancer. Such treatment is called curative radiotherapy. To be curative, the treatment must eradicate every cancer cell or prevent them from growing and multiplying. High doses are often required when the aim of the radiation therapy treatment is to cure. Radiation therapy may also be used to relieve cancer symptoms, even when cure is not possible. This type of treatment is called palliative radiotherapy.
How is radiation therapy given?
There are two main types of radiation therapy- external beam radiation therapy and radioactive implants. With external beam radiation therapy, a machine is used to direct the radiation to the cancer through the skin. Most of the patients who are treated with radiation therapy are treated with external beam irradiation.
With radioactive implants, radioactive sources are placed inside the body within or next to the tumour. Radioactive implants are often used to treat well-localised cancers because a greater dose of radiation can be given to the tumour with less dose to surrounding healthy tissues. It is not unusual for a patient to receive a combination of external beam radiation therapy followed by a radioactive implant.
Flow Chart of Radiation Therapy
Consultation
 When you some to the clinic, a radiation oncologist will review your current problem, past medical history, past surgical history, family history, medications, allergies, lifestyle and an organ system by organ system audit making use of any relevant x-rays and lab tests that you already have had. He/she will also perform a physical examination that will then to assess the extent of your problem and judge your general physical condition to estimate any influence it may have over your response to radiation therapy.
When you some to the clinic, a radiation oncologist will review your current problem, past medical history, past surgical history, family history, medications, allergies, lifestyle and an organ system by organ system audit making use of any relevant x-rays and lab tests that you already have had. He/she will also perform a physical examination that will then to assess the extent of your problem and judge your general physical condition to estimate any influence it may have over your response to radiation therapy.
Simulation
The simulation process will help the radiation team plan a course of treatment designed especially for you. The radiation oncologist uses the x-rays images and the information gathered during the simulation to design and individualise your treatment plan.
 Simulators are very precise machines that can duplicate the geometry of different types of treatment machines and by fluoroscopy and x-ray pictures allow us to visualise important structures inside patients. This information is translated into aiming points, distances and angles. With you lying on the simulator couch and with the use
Simulators are very precise machines that can duplicate the geometry of different types of treatment machines and by fluoroscopy and x-ray pictures allow us to visualise important structures inside patients. This information is translated into aiming points, distances and angles. With you lying on the simulator couch and with the use of light and laser projection systems we will place marks on your skin or on individually constructed immobilisation devices that will help level and position you in 3-dimensional space. Marking may be tattooed on the skin. Immobilisation devices will be constructed from one or more materials including thermally shaped plastics, vacuum forming beanbags, and plaster casts. You may need an appointment with the mould room for making of your immobilisation device.
of light and laser projection systems we will place marks on your skin or on individually constructed immobilisation devices that will help level and position you in 3-dimensional space. Marking may be tattooed on the skin. Immobilisation devices will be constructed from one or more materials including thermally shaped plastics, vacuum forming beanbags, and plaster casts. You may need an appointment with the mould room for making of your immobilisation device.
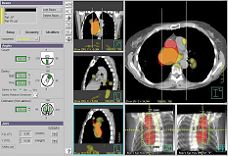
Treatment Planning
The treatment planning team includes the radiation oncologist, radiographer and physicist. Using all available information, including that obtained from simulation, the final plan will determine the type of radiation, its size and shape and the number of radiation beams, and how much radiation is given through each beam. Radiation beams must be shaped to match their intended targets with the collimator jaws. Depending on the desired shape, additional blocking of the beam may be required. The treatment planning computer then calculates the desired dose distribution taking into account the sparing of normal healthy tissue and the tolerance of the patient as a whole. The radiation oncologist approved the final plan and the treatment parameters are printed in a hardcopy with the electronic version sent to the treatment machine treatment record system via the hospital network.
 |
 |
Machine Quality Assurance
Treatment Routine
Monitoring Your Progress
Possible Side Effects
You are not radioactive and it is not harmful to anyone around you unless you have an implant of radioactive seeds, wire or ingested/infused radiopharmaceuticals. It is not unusual to feel tired during the time you are receiving radiation therapy. Many patients find it helpful to take an afternoon nap or get more sleep each night. Usually, you can continue your normal lifestyle. Your body is your best guide.
Treatment Modalities
Photon Beam Therapy
 Photons are x-rays produced with a machine like the linearaccelerator or gamma rays from a Cobalt-60 unit. These highenergy photons are capable of penetrating deeply into tissues toreach deep seated tumours while actually delivering lessradiation dose to superficial tissues such as the skin. The actualphoton energy chosen to treat a tumour depends on thecharacteristics of the tumour, patient and treatment technique. The linear accelerator is capable of rotating around a patientlying on a treatment couch, treating the tumour from severalangles More often, two or more intersecting beams of radiationare directed at a tumour from different directions.
Photons are x-rays produced with a machine like the linearaccelerator or gamma rays from a Cobalt-60 unit. These highenergy photons are capable of penetrating deeply into tissues toreach deep seated tumours while actually delivering lessradiation dose to superficial tissues such as the skin. The actualphoton energy chosen to treat a tumour depends on thecharacteristics of the tumour, patient and treatment technique. The linear accelerator is capable of rotating around a patientlying on a treatment couch, treating the tumour from severalangles More often, two or more intersecting beams of radiationare directed at a tumour from different directions.
Electron Beam Therapy
Most patients are treated with x-ray beams produced by linear accelerators. These accelerators can also produce a beam of high-energy electrons which penetrate into tissue to a much more limited depth than x-rays. The treatment effect of electrons and x-rays is considered identical. Electron beams can be used for treating superficial tissues such as skin, lymph nodes and whenever it is preferable to deliver a higher radiation dose superficially and relatively less dose to deeper tissues.
Conformal Three Dimensional Radiotherapy
The objective of radiation therapy is to deliver a high dose to the tumour to achieve a high level of local control while keeping the dose to neighboring healthy tissues as low as possible.
 In conventional radiation therapy, the dose distribution can only be evaluated in a single, usually transverse, central plan although the tumour and the neighboring tissues bear complex three-dimensional relationships to one another. To ensure that the tumour receives an adequate dose, a margin is included around the tumour volume to account for the uncertainties in tumour delineation and dosimetry and deviations due to patient movement. This safety margin often limits the delivery of a high dose to the target volume because of the tolerance of the normal tissues included in the irradiation.Three dimensional (3D) conformal radiation therapy is a sophisticated irradiation technique which allows a high dose delivered to the tumour while keeping the dose to the adjacent normal tissues below tolerance. 3D conformal therapy combines modern imaging technology (such as CT and MRI) for accurate tumour delineation with state-of-the-art computer planning systems for treatment planning and the latest development in linear accelerator technology such as the multileaf collimators for precise and sophisticated dose delivery.
In conventional radiation therapy, the dose distribution can only be evaluated in a single, usually transverse, central plan although the tumour and the neighboring tissues bear complex three-dimensional relationships to one another. To ensure that the tumour receives an adequate dose, a margin is included around the tumour volume to account for the uncertainties in tumour delineation and dosimetry and deviations due to patient movement. This safety margin often limits the delivery of a high dose to the target volume because of the tolerance of the normal tissues included in the irradiation.Three dimensional (3D) conformal radiation therapy is a sophisticated irradiation technique which allows a high dose delivered to the tumour while keeping the dose to the adjacent normal tissues below tolerance. 3D conformal therapy combines modern imaging technology (such as CT and MRI) for accurate tumour delineation with state-of-the-art computer planning systems for treatment planning and the latest development in linear accelerator technology such as the multileaf collimators for precise and sophisticated dose delivery.
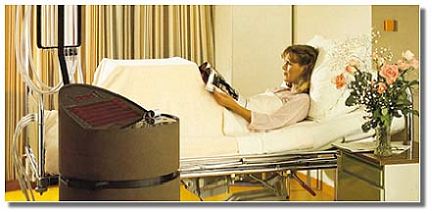
High Dose Rate (HDR) Remote Afterloading Brachytherapy
 The radioactive source transfer unit employs a high-activity miniature iridium-192 seed attached to the end of a steel wire to deliver the radiation treatment under computer control. In this way, the position of the source within the patient's body and the length of time it remains can be accurately controlled. Applicators for cancer of the cervix and breast Various devices, or applicators, are used to provide access for the radiation source into the area to be treated within a human body. Different applicator designs are available for treatment of tumours or other lesions located at different areas of the body. The applicators are placed within the patient (who is an esthetised if necessary, depending on the site to be treated). To prepare for the treatment, non-radioactive markers are placed inside each applicator, and X ray films are taken to visualise the actual setup.
The radioactive source transfer unit employs a high-activity miniature iridium-192 seed attached to the end of a steel wire to deliver the radiation treatment under computer control. In this way, the position of the source within the patient's body and the length of time it remains can be accurately controlled. Applicators for cancer of the cervix and breast Various devices, or applicators, are used to provide access for the radiation source into the area to be treated within a human body. Different applicator designs are available for treatment of tumours or other lesions located at different areas of the body. The applicators are placed within the patient (who is an esthetised if necessary, depending on the site to be treated). To prepare for the treatment, non-radioactive markers are placed inside each applicator, and X ray films are taken to visualise the actual setup.
Computer radiation dose calculations are done by the medical physicist who also performs machine quality assurance tests. After the treatment plan has been approved by the radiation oncologist, the applicators are then connected to the HDR brachytherapy unit and treatment is delivered.  Each treatment takes about 30-60 minutes, including treatment planning time. The actual radioactive application only lasts for about 5-15 minutes. HDR brachytherapy is customised to each patient, so an optimised radiation dose is applied within the precise contours of the target. The implants are temporary and treatment is given during a few concentrated sessions lasting minutes to hours as opposed to low dose rate (LDR) brachytherapy which typically requires that the radioactive sources remain in the patient for several days while the patient stays in the hospital.
Each treatment takes about 30-60 minutes, including treatment planning time. The actual radioactive application only lasts for about 5-15 minutes. HDR brachytherapy is customised to each patient, so an optimised radiation dose is applied within the precise contours of the target. The implants are temporary and treatment is given during a few concentrated sessions lasting minutes to hours as opposed to low dose rate (LDR) brachytherapy which typically requires that the radioactive sources remain in the patient for several days while the patient stays in the hospital.
 |
 |
||||
| Applicators for cancer of the cervix and breast | |||||
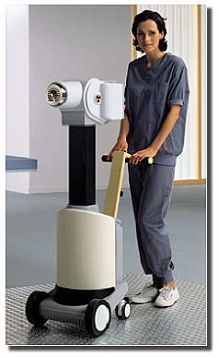
Low Dose Rate (LDR) Remote Afterloading Brachytherapy
 For some diseases such as cancers of the cervix, uterus or vagina, the radiation oncologist may choose to administer low dose rate brachytherapy. The radioactive sources are in the form of small caesium pellets which will be delivered remotely with the transfer unit into the hollow applicators which have previously been inserted into the body cavity by the radiation oncologist. The treatment time may last for a couple of days depending on the clinical indications.
For some diseases such as cancers of the cervix, uterus or vagina, the radiation oncologist may choose to administer low dose rate brachytherapy. The radioactive sources are in the form of small caesium pellets which will be delivered remotely with the transfer unit into the hollow applicators which have previously been inserted into the body cavity by the radiation oncologist. The treatment time may last for a couple of days depending on the clinical indications.
Manual Implants
Manual implants usually employ low-activity (hence low dose rate) material and could be either temporarily or permanently inserted into the body tissues or body cavity. The sources are usually much smaller than the LDR caesium pellets and may be in the form of seeds, wire, hairpins or needles etc.
Special Procedures
Stereotactic Radiosurgery
Radiosurgery is a treatment technique to deliver sharply focused beams of radiation to intracranial targets. Multiple small beams of radiation intersect at a focal point to create a small ball or sphere of high dose radiation which then could be targeted with a high degree of precision to an intracranial lesion using a head frame unit attached to the skull. The term "stereotactic" refers to the targeting mechanisms which employ computerised tomography (CT), magnetic resonance imaging (MRI), or angiography to direct the radiosurgery beams in 3D. Stereotactic therapy is used as both a single dose radiation treatment, stereotactic radiosurgery (SRS), and multiple fraction of smaller doses called stereotactic radiotherapy, (SRT).
There are currently two types of technology for the delivery of SRS: Gamma Knife, which employs an array of over 200 concentrically positioned sources of cobalt-60 to aim at the intracranial target. Another approach is to use a linear accelerator (with small treatment cone or miniature collimators) to create a sphere of radiation by aiming an array of intersecting non-coplanar arc beams of radiation.
Malignant brain tumour, meningiomas, orbital tumours, arteriovenous malformations (AVM's), acoustic neuromas, metastatic tumours to the brain, pituitary tumours and brain stem tumours, skull base tumours, head and neck tumours including nasopharyngeal carcinoma and selected recurrent tumours near the skull base are treated with these techniques.
Intensity Modulated Radiation Therapy
Intensity Modulated Radiation Therapy (IMRT) is a sophisticated technology that can deliver a high dose of radiation to a tumour while sparing surrounding healthy normal tissues with good conformality.
The fundamental difference between conventional conformal radiation therapy and IMRT is beam intensity; in conventional radiation therapy, the beam intensity is uniform, but in IMRT, the beam intensity is varied across the treatment field. During IMRT treatment, when the tumour is the thickest,the beam intensity is at its maximum, and when the tumour is the thinnest, the intensity is at its minimum. This technique can also spare adjacent of overlying healthy tissues. Instead of the patient being treated with a single, large uniform beam, the patient is treated with a large number of smaller beamlets, each with different intensities or amounts of radiation.
IMRT allows the radiation oncologist to conform the radiation dose to difficult tumour volumes, yet spare eloquent areas -- for instance, treating a tumour that has wrapped itself around the spinal cord. IMRT is similar to conformal therapy, which is practiced in many radiation oncology centers, but conformal therapy is limited to a geometric shaping of the beam with no intensity modulations across the field.
When a tumour is not well separated geometrically from surrounding organs, adding modulation to the geometric shaping of the beam is more effective in conforming the dose to a tumour while minimising the dose to normal surrounding structures. This way, an optimised treatment plan can be created for a given tumour of any size, shape or anatomical location.
Total Body Irradiation (TBI)
Total body irradiation is often used in bone marrow transplantation. This procedure may be considered as an x-ray bath and aids in the transplant process. In this procedure the medical physicist must carefully take into account the patent’s thickness, size, shape, and treatment position. This information is used by the medical physicist to design custom shielding to protect vital organs, and to determine how long the beam should remain "on" to deliver the dose prescribed by your radiation oncologist.
Total Skin Irradiation (TSI)
There are few conditions that require a radiation oncologist to irradiate a patient’s entire skin surface. The most common entity is cutaneous lymphoma or mycosis fungoides. This disease entity involves malignant lymphocytes that have a propensity for lodging in the patient’s skin and causing tremendous discomfort with agonising itching and generalised skin irritation. This particular disease does not respond well to chemotherapy. In contrast, it is readily sensitive to radiation therapy.
Mycosis Fungoides presents several distinct problems that require significant attention to detail. The desire is to treat the skin surface and not damage underlying organs and tissue. For this we use a type of radiation called electrons. They have the unique property of traveling only a short distance in tissue.This creates several inherent problems. Skin or other structures shield much of one’s skin surface. For example, the region between the thighs, perianal regions, bilateral axillae and soles of the feet are normally shielded. Multiple mini radiation detection devices called TLDs are placed on the skin to allow us to accurately measure the radiation dose to multiple sites. Those sites underdosed can be given as mall boost of radiation to ensure all areas receive the prescribed dose of radiation therapy.
Who’s who in radiation therapy
Medical Physicist
Medical physicist is a health care professional. He/she is responsible for developing and maintaining physics support in the practice in medicine. In particular, medical physicists work mostly in the radiation oncology, x-ray and nuclear medicine departments where they perform quality assurance work on equipment and radioactive materials used and the procedures of diagnostic and therapy deliveries.
Radiation Oncologist
A radiation oncologist is a physician trained in the treatment of cancer with radiation. He/she is the person in charge of your treatment and follow-up and responsible to answer any concerns you may have about your care. Oncology residents, who are physicians in training, also may participate in your care under the direct supervision of your radiation oncologist.
Oncology Nursing
The radiation oncology nurses, with special backgrounds in all aspects of cancer care, provide a full array of nursing services, including emotional and physical support. They provide ongoing clinical supervision to support all patients undergoing therapy. The nurses are also involved in research projects and the development of educational groups to assist the patient as they undergo treatment.
Radiographers
Radiographers administer the daily radiation treatments and working under your oncologist's prescription or treatment plan. Some radiographers also perform simulation and treatment planning.
Support Services
To assist with the emotional aspects of cancer and treatment, social workers and patient support groups are available to you and your family to talk about fears and expectations. Nutrition specialists will offer dietary advice, and the home care and hospice programs provide support, nursing care and in-home services.
FAQ
How does radiation therapy work?
The purpose of radiation therapy is to kill cancer cells. Radiation affects all rapidly dividing cells, both normal and abnormal. Treatment is designed to maximise the radiation dose to tumour cells while minimising harmful effects to normal tissue. Normal cells have a greater ability to repair themselves than do cancer cells. Because it is impossible to shield all normal tissue, some side effects may occur. Your doctor and nurse will discuss the specific side effects with you.
Am I radioactive?
No, you are not radioactive and you will not be a danger to anyone during (unless with an implant) or after your course of radiation therapy.
Will I feel the radiation?
Similar to having a routine X-ray, there is no sensation from the radiation.
Will I lose my hair?
You will lose hair only in the area that is receiving radiation therapy. The hair on your head will not be affected unless you are receiving therapy to your head. This loss usually is not permanent. Be sure to ask your doctor or primary nurse any additional questions about hair loss.
Will my skin be burned?
Skin reactions are a common side effect of radiation therapy. The skin within the treatment area may look and feel like sunburn. You may experience dryness, irritation, tanning or peeling. These conditions are temporary and will heal after treatments are completed. Your nurse will review with you how to care for your skin during and after your course of radiation treatments.
Will I feel tired?
You may tire easily during your course of radiation therapy and need to rest more often. The degree of fatigue varies widely from patient to patient and may persist for a few weeks after completion of treatment. If you have questions ask your nurse or doctor.
Can radiation therapy cause another cancer?
Patients who have one cancer have an increased risk of having a second cancer later. It does not matter how their first tumour was treated. The risk of developing a second minor because of radiation therapy is very low.
Why does radiation therapy take so long?
Normal cells are able to repair DNA damage far better after small doses of radiation than after large doses. In fact, experience with many thousands of patients treated over many decades has shown us that we can minimise side effects by dividing a large total dose of radiation into many smaller daily doses delivered over several weeks rather than giving a few massive doses in several days. Between each of your daily doses, the normal cells are repairing their damaged DNA. This results in fewer side effects. Although it seems very inconvenient to give treatment over such a long period of time, this is the only way to deliver enough total radiation to permanently destroy your cancer without also permanently hurting normal tissues.
Can I Miss a Treatment?
Unless a treatment break is prescribed by your doctor, it is preferable to receive all of your radiation therapy treatments in sequence. Occasionally, because of machine malfunction, a treatment may be canceled. In this case a make-up treatment will be added at the end of your originally scheduled course. The same is true if you cannot come in for a scheduled treatment. Please notify the nurse and/or technologist by telephone if you have to miss an appointment.
Can I receive radiation treatments more than once?
Generally a patient can receive radiation therapy to a given area only once. This is because further radiation therapy to that same area might cause unacceptable side effects or permanent damage.Occasionally, if the radiation tolerance has not been exceeded, someone can receive more radiation even to an area that was already treated. Because the effects of radiation are local, most patients can receive radiation to another part of the body just as if they had no previous radiation.
How does taking radiation and chemotherapy at the same time affect my body?
For certain types of cancer, a combination of radiation and chemotherapy are more effective than either one alone. Chemotherapy is a systemic treatment which is acting on the whole body as it travels through the bloodstream. When it is given at the same time as radiation, it often increases the effect of radiation on cancer cells. Unfortunately, sometimes there is also an increase in side effects when both treatments are given together. The exact type of chemotherapy used depends on what kind of cancer is being treated.
What are clinical trials?
Radiation oncologists, physicists and others continue to explore new ways to treat the cancer patient effectively with radiation and radioactive sources. The practice of radiation oncology continues to grow and change. Cancer specialists are conducting studies now to determine what treatment is best for each cancer patient. These studies are called "clinical trials" or "treatment protocols." Most large clinical trials compare standard treatment to a treatment that cancer experts think might be better. All patients who participate in clinical trials are carefully monitored to make sure they are getting quality care.Cancer patients should talk to their doctor about clinical trials before they choose treatment.
Glossary
A | B | C | D | E | F | H | I | L | M | P | R | S | T
A
Alpha Cradle: A treatment device that is custom-made from a foam substance, and is placed on the patient during a radiation treatment for the purpose of immobilising and/or positioning the patient.
Arc: refers to a radiation beam that is not stationary, that is, the beam moves around an axis is a curvedpath during the treatment. Also called a rotation.
B
Barium: a radiographic contrast agent used in radiation oncology during simulation to visualise specific organs (e.g., esophagus, stomach, bowel).
Bite Block: a treatment device that is placed in the patient's mouth during treatment for the purpose of positioning oral structures in the radiation beam. Also called a mouthbite or stent.
Block: a treatment device made from a lead alloy that is placed in part of the radiation beam by attaching it to the treatment unit on a plastic tray for the purpose of preventing the beam form entering a portion of the body. A block is used either to spare sensitive or uninvolved body organs.
Brachytherapy: refers to radiation therapy given form a very short distance form the radiation source,that is, radioactive needles, seeds, liquid, or tubes are placed inside a body cavity or organ or on the skin.
C
Cesium: an element made radioactive and used in Brachytherapy, gene rally in the form of either needles or tubes.
Cone Down Boost: An additional radiation dose delivered to a more narrowly defined port.
Conformal Radiation Therapy: Conformal therapy allows for the radiation beam to conform to the tumour's contour and size, reducing side effects and increasing cure rates.
Contrast Material: liquid or gel -type agents introduced into a body cavity for the purpose ofvisualising specific organs.
Computerised Tomography(CT): a specialised x-ray taken by a "CT" scanner that takes "slices" of abody part.
D
Dosimetry: the measurement of radiation dose.
Dummy: a radioactive source that is made to simulate the size and appearance of a radioactive source on a verification X-Ray. It is used to prevent radiation exposure to the healthcare workers during the planning phase for a Brachytherapy treatment.
E
Electron Therapy: A form of radiation therapy in which the radiation oncologist selects a specific shallow depth and treats only this area without treating structures above and below this interest point.
F
Field: a specific area of the body designated for treatment. Generally a field is named by the part of the body that the radiation beam enters
Fraction: Pertaining to a portion of the whole treatment course. Generally a fraction can be described as a treatment visit. Most radiation treatment courses are "fractionated" i.e., the total prescribed dose is divided into several treatment visits or fractions. e.g., A total dose of 3000 cGy may be divided into 10 treatment visits or fractions of 300 cGy each.
H
HDR: High dose rate. Refers to a particular method of delivering a dose for Brachytherapy in which the dose rate is much higher than in conventional Brachytherapy.
Hyperfractionation: the delivery of treatments more than once per day. In radiation oncology this term generally refers to two or three treatment visits per day with a separation of at least six hours between treatments.
Hyperthermia: the use of heat to help to intensify the effects of radiation.
I
Implant: refers to the placement of radioactive sources within the body.
Intra-operative: refers to radiation treatment delivered while the patient is undergoing surgery.
Interstitial: relating to the spaces within an organ or tissue. Refers to the placement of radioactive sources within the tissues of the body. i.e., breast, tongue, lip, brain prostate. In contrast to intracavitary
Intracavitary: Within a body cavity. Refers to the placement of radioactive sources within a body cavity. i.e., cervix, uterus, esophagus. In contrast to interstitial.
Iodine: an element made' radioactive and used in Brachytherapy. A non-radioactive form of this element may be used as a radiographic contrast agent during simulation to visualise specific organs.
Iridium: an element made radioactive for the use in Brachytherapy.
L
Linear Accelerator: a teletherapy machine that produces radiation by moving particles very rapidly(accelerating) along a straight path (linear) and then hitting a target. Linear accelerators are manufactures with the capability of having either a single energy or a dual energy. The higher the energy, the deeper the beam reaches inside the body.
M
Mantle: specialised radiation treatment field to the chest in which the chest and neck lymph system istreated and the other areas are spared by blocks.
MRI: Magnetic resonance image. a special diagnostic image taken by an "MRI" scanner that takes"slices" of a body part.
P
Photon Treatment: a form of radiation therapy in which the radiation oncologist selects a specific radiation energy appropriate for the patient's body size and depth of the tumour(the higher the energy the deeper the beam reaches inside the body. Contrary to electron treatment, photon treatment deposits a radiation dose above and below the tumour site.
Physicist: the radiation oncology health professional whose primary duty is to oversee the quality assurance aspect of a patient's treatment. Some duties may include calibration and overseeing of the radiation equipment and overseeing charting.
Port Film: a radiographic image captured on film that shows the prescribed treatment area (port). A port film is different form an X-Ray in that a port film is taken for the purpose of a record of the body site treated with radiation and is generally not used as a diagnostic tool.
R
Radiation Oncologist: the radiation oncology health professional who is a physician who prescribes and oversees a course of radiation therapy.
Radiographer: the radiation oncology health professional who carries out the radiation prescription by using a radiation machine. Some radiographers also perform treatment simulations and planning.
Remote Afterloading: refers to Brachytherapy delivered by loading the radioactive sources into the patient form a remote location.
Ribbons: refers to the temporary interstitial placement of radioactive elements.
S
Set Up: a procedure whereby the physical parameters (i.e. body position, machine angle) are defined before the treatment is given. A set up may be done on a simulator, radiation therapy treatment unit, or a diagnostic X-Ray unit.
Shield: a treatment device,that' generally is custom made which spares radiation to a specific body area.
Simulation: a radiation oncology procedure, performed prior to treatment, carried out on a dedicated"simulator", radiation therapy treatment unit, or diagnostic X-Ray unit during which the treatment parameters (patient position, field size, etc.) are defined. This procedure "simulates" the actual treatment without delivering the radiation dose.
Simulator: a treatment planning machine whose physical parameters mimics those of an actual radiation treatment unit, but without the high radiation beam energy that actually delivers a treatment.
Sources: refers to intracavitary placement or permanent interstitial placement of radioactive elements.In contrast to ribbons.
Stereotactic: refers to a method of precisely locating areas in the brain.
T
TBI: total body irradiation. Refers to a radiation beam that encompasses the entire body.
Treatment: specifically, the radiation beam time for each field or more generally all ports that are treated in one visit.
Treatment Plan: the process whereby the radiation oncologist provides interpretation of tests, tumour localisation, treatment time/dose determination, choice of treatment modalities, determination of number and size of treatment ports, selection of treatment devices, etc.